
PREPARING FOR THE DAY OF SURGERY
Mohs surgery is a minor surgical procedure performed on an outpatient basis in our office, so there is usually no special preparation required before Mohs surgery.
We recommend getting a good night’s rest so you are well-rested and having a good breakfast on the morning of the surgery. Unless it is medically necessary, we ask that you do NOT take aspirin, vitamin E, vitamin C, or ibuprofen (naprosyn, Motrin, Advil, Aleve) for 14 days prior to surgery. Be sure to CONTINUE TAKING ALL of your other usual medications including PLAVIX and COUMADIN. We also require that you do not drink any alcohol for 3 days prior to surgery, since this will cause more bleeding. Smoking also delays the healing process and should be stopped two week prior to surgery and for one week afterwards.
Please shower and shampoo your hair the night before or the morning of surgery, as your wound and bandages must remain dry for the first 24-48 hours. We also suggest you wear loose fitting, comfortable clothing—a button-down shirt is best so you don’t have to pull your shirt over the bandages. You may want to bring a sweater or jacket, as the waiting area is often cool. Please do not wear any makeup, perfume, or jewelry. The length of the surgery varies greatly depending on the size and location of the skin cancer. You should plan on spending most of the day with us. It is wise to bring a book or magazine to read and some snacks/lunch in case you are hungry. Also, because the day may prove to be quite tiring, it is advisable to have someone accompany you on the day of surgery to provide companionship and to drive you home.
Your referring physician may request that you have a preoperative consultation visit to evaluate the need for Mohs surgery. At this visit, the technique will be discussed in detail and you will meet the “team” performing the surgery. If you are traveling a great distance and/or are being referred by a physician familiar with the technique, you may be referred directly for Mohs surgery without a preoperative visit. When your appointment is scheduled, our nurse coordinator will discuss with you your pertinent medical history and give you instructions regarding any medications you are taking.
WHAT TO EXPECT ON THE DAY OF SURGERY
REGISTRATION: Your appointment has purposely been scheduled early in the day. Upon your arrival you should check in at the Reception Desk. A map and travel instructions are included with this booklet. The cost of Mohs surgery is covered by most insurance carriers. Please be prepared to give insurance information to our billing office and bring with you any forms that may need processing.
MEET THE TEAM: When the surgical suite becomes available, you will be escorted by our surgical nurse to your room. Photographs will be taken and we will obtain written consent for the procedure. If you have not had a consultation visit, any questions your may have will be carefully answered by members of our highly trained team of medical personnel. In addition to your Mohs surgeon, our “Mohs team” consists of a nurse, a histotechnician, a procedural dermatology fellow and dermatology residents. We function as a team to provide the highest quality medical care. The fellow is a board certified dermatologist who is undergoing further surgical training in the Mohs surgery technique. Your nurse is an important part of the team who will help answer your questions, respond to your anxieties, assist in surgery, and instruct you in dressings and wound care after the surgery is performed. A technician, who you may not even meet, performs the essential task of preparing the tissue slides, which are examined under a microscope by the physician during the procedure. When all your questions have been addressed and your records reviewed, the surgery will begin.
THE MOHS PROCEDURE: The Mohs surgical process involves repeated “stages” of surgical excisions followed by microscopic examination of the tissue to assess if any tumor cells remain. Each stage can take approximately one hour. Only 10-20 minutes of that time is spent in the actual surgical procedure, with the remaining time being required for slide preparation and interpretation.
Some tumors that appear small on clinical exam may have extensive invasion underneath normal appearing skin, resulting in a larger surgical defect than would be expected. It is therefore impossible to predict in advance the number of stages necessary or the time that will be required to adequately treat your cancer. As Mohs surgery is used to treat complex skin cancers, approximately half of all treated tumors require 2 or more stages for complete excision
Step 1: Anesthesia
The area around the skin cancer will be numbed with a local anesthetic similar to when you had your original biopsy. General anesthesia is not required for Mohs micrographic surgery.
|
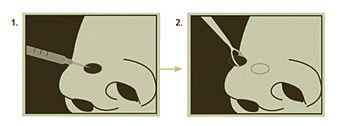 An injection numbs the area. The visible portion of the tumor is removed.
An injection numbs the area. The visible portion of the tumor is removed.
|
Step 2: Stage I – Removal of visible tumor
Once the skin has been completely numbed, the tumor is gently scraped with a curette, a semi-sharp, scoop-shaped instrument. This helps define the margin of the tumor. The first thin, saucer shaped “layer” of tissue is then surgically removed by the Mohs surgeon. Electrocautery may be used to stop the bleeding. This process takes approximately 10-20 minutes.
|
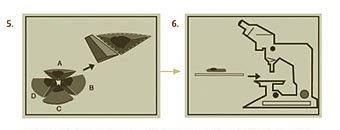
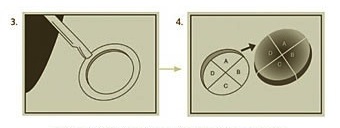
Step 3: Mapping the tumor
Once a “layer’ of tissue has been removed, a “map” or drawing of the tissue and its orientation to local landmarks (e.g. nose, cheek, etc) is made to serve as a guide to the precise location of the tumor. The tissue is labeled and color-coded to correlate with its position on the map. The tissue sections are processed and then examined by the surgeon to thoroughly evaluate for evidence of remaining cancer cells. It takes approximately 60-90 minutes to process, stain and examine a tissue section. During this processing period, your wound will be bandaged and you may leave the operative suite.
|
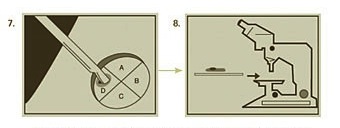
Step 4: Additional stages – Ensuring all cancer cells are removed
If any section of the tissue demonstrates cancer cells at the margin, the surgeon returns to that specific area of the tumor, as indicated by the map, and removes another thin layer of tissue only from the precise area where cancer cells were detected. The newly excised tissue is again mapped, color-coded, processed and examined for additional cancer cells. If microscopic analysis still shows evidence of disease, the process continues layer-by layer until the cancer is completely removed. By beginning early in the morning, Mohs surgery is generally finished in one day. Sometimes, however, a tumor may be extensive enough to necessitate continuing surgery a second day.
RECONSTRUCTION: Mohs surgeons are experts in the reconstruction of skin defects. Reconstruction is individualized to preserve normal function and maximize aesthetic outcome. The best method of repairing the wound is determined only after the cancer is completely removed, as the final defect cannot be predicted prior to surgery. Stitches may be used to close the wound side-to-side, or a skin graft or a flap may be designed. Sometimes, a wound may be allowed to heal naturally.
- Healing by spontaneous granulation involves letting the wound heal by itself naturally. Experience has taught us that there are certain areas of the body where nature will heal a wound as nicely as any further reconstruction. Healing time is approximately 3-6 weeks and requires daily care.
- Closing the wound with stitches is often performed on a small lesion. This involves some adjustment of the wound and sewing the skin edges together. This procedure speeds healing and can offer a good cosmetic result. For example, the scar can be hidden in a wrinkle line.
- Skin Grafts involve covering a surgical wound with skin from another area of the body. The donor site is then sutured together to provide a good cosmetic result. Skin grafts may require a “bolster” dressing–a special bandage which is sutured over the skin graft. The “bolster” dressing will remain over the graft for a week or until sutures are removed.
- Skin flaps involve movement of adjacent, healthy tissue to cover a surgical site. Where practical, they are chosen because of the excellent cosmetic match of nearby skin.
Almost all reconstructions are performed here in our facility. In rare cases, when the wound is quite extensive or when removal of the tumor results in functional impairment, we may recommend that you visit one of several consultant facial plastic or plastic surgeons for reconstruction. This may take place on the same day as your Mohs procedure or on subsequent days.
WHAT TO EXPECT AFTER THE SURGERY
Wound Care: Detailed written instructions on wound care will be given to you upon completion of the surgery. Essentially, you will leave the original bandage on for the first 24 hours. Then, on a daily basis until the stitches are removed, you will gently clean the wound using soap and water, then place an ointment (Vaseline or Aquaphor) on the wound, and cover it with a dressing. Keep the wound CLEAN, MOIST, and COVERED. It is very important to keep the wound moist with ointment, and not to let it dry out. When a wound dries and scabs, it will take longer to heal and form a much more noticeable scar.
Pain: Most patients report minimal amount of discomfort the first day or two following surgery. This discomfort usually responds readily to Tylenol. Due to its potential to cause bleeding, we request that you do not take aspirin or ibuprofen for pain control for three days following surgery. In some cases, you may be prescribed a stronger pain medication. There may also be a normal sensation of itching or tightness that is expected during the healing process.
Exercise and Activity: Be aware that you should avoid physical activities such as bending, lifting, or exercise for at least one week following your procedure. We recommend that you refrain from cleaning the house and lifting heavy items. Please arrange your schedule in advance to avoid these activities.
Healing Process: Often patients will have “black and blue” marks and swelling around the site of surgery. This reaction is particularly exuberant around the eyes, especially if surgery was performed near the eyes, forehead or nose. This usually gets worse for the first three days after surgery, and then slowly begins to improve. The use of ice packs during the first 48 hours will help reduce swelling and bruising.
Suture Removal: You will be seen for suture removal 7-14 days after surgery. Most patients need to return for one or two more visits to make sure everything is healing according to schedule. The importance of the follow-up visits should not be underestimated.
RISKS OF SURGERY
Because each patient is unique, it is impossible to discuss all of the complications and risks in this brochure. Remember, every surgical procedure produces some form of a scar. Although every attempt will be made to minimize the scar, the extent of the scarring depends on the location, size, and depth of the skin cancer, and the healing properties of each patient. We will make every effort to obtain optimal cosmetic results, but our primary goal is to remove the entire cancer. Keep in mind that the scarring associated with Mohs’ surgery is generally far less than with other surgical treatment of skin cancers.
Typical risks for Mohs surgery are discussed below, but it is important to note that these are the same risks involved in any routine skin surgery. Your Mohs surgeon will discuss any additional potential problems associated with your particular case on the day of your surgery. Please understand that these are the exception, not the rule:
- The surgical wound created by removal of the skin cancer may be larger than anticipated. Also, the elastic properties of the skin cause wound gaping so that the size of the hole in the skin is always larger than the size of the piece of skin that was removed. There is no way to predict prior to surgery the exact size of the final surgical wound. Also, the reconstructive surgery may be larger or more extensive than anticipated in order to avoid puckering or pulling on vital structures. Typically, a linear scar must be 3 times longer than the width of the surgical wound to avoid lumpiness of the scar.
- Although all surgery leaves a scar, sometimes this scar call be thickened, spread, depressed or painful. This often improves over time and attempts may be made to correct the problem. The scar will continue to improve for 8-16 months. After the first month, the area should be gently massaged if it feels thick or lumpy. The scar can be minimized by the proper care of your wound.
- Poor wound healing may occur, despite our best efforts. Many things influence how well you will heal (location of the tumor, bleeding, medications, poor physical condition, smoking, diabetes or other medical problems). Healing may be slow (particularly on the legs and scalp) or the wound may reopen. Flaps or skin grafts used to repair a defect may at times fail. Under these uncommon circumstances, the wound will usually be left to heal on its own.
- You may experience some numbness around the area that was operated on. The lips, forehead, and scalp are areas where temporary numbness may occur. There are many small nerves that carry sensation to the skin. Some of these may be cut during surgery, and it may take 6-12 months before full sensation returns. Rarely the skin cancer involves larger nerves. When these are cut, the loss of sensation or muscle weakness may be permanent. Prior to surgery, the doctor will discuss with you any major nerves which may be near your tumor.
- Although temporary swelling and bruising are common after surgery, long lasting or permanent swelling is uncommon. Swelling generally resolves in days, but may take weeks to improve.
- Rarely, wounds become infected and require antibiotic treatment. If you are at particular risk for infection, you may be given antibiotics prior to surgery or after completing surgery.
- Bleeding from the wound may be excessive during surgery. While uncommon, if bleeding occurs after surgery under a sutured wound, skin flap or skin graft, it may impair healing.
- There may be adverse reactions to medications used before, during or after surgery We will carefully screen you for any history of problems with medications.
- There is a small chance that your tumor may regrow after surgery. Previously treated tumors and large, long-standing tumors have a greater chance of recurrence than smaller tumors which have never before been treated.
- Smoking before or after surgery can lead to complications. Minimize smoking one week prior to and after surgery if at all possible, but it is best not to smoke at all during this time.
Wound healing is a very complex process. Once your stitches are removed, the wound undergoes significant remodeling to form new collagen. Often the scar is initially red and lumpy, but with time, this generally will resolve. It can often time take weeks or months before final judgment of results can be made. Be patient during the healing process.
If you have any questions about our services, please contact us today at (615) 266-3376 (DERM).